表1 2组孕妇妊娠结局和胎儿体质量的对比

组 别产妇数/例新生儿出生体质量m/g大胎儿小胎儿分娩孕周/周两胎儿体质量差m/g观察组402130.8±350.61)1520.0±452.81)34.2±4.61)27.4±2.51)对照组402572.5±508.42358.0±462.337.0±3.48.0±1.5
曾琳芮
(成都市第七人民医院 妇产科,四川 成都 610041)
【摘要】目的:探析不同类型单绒毛膜双羊膜囊(MCDA)双胎妊娠选择性宫内生长受限(sIUGR)胎儿的妊娠结局及预后情况。方法:选取我院2010年6月至2015年6月收治的MCDA并发sIUGR孕妇40例(80胎)作为观察组,同时根据脐动脉血流频谱分型将其细分为Ⅰ型组(20例)、Ⅱ型组(12例)和Ⅲ型组(8例)。另选取同期无合并症的MCDA孕妇40例(80胎)作为对照组。对比2组及3种类型sIUGR之间胎儿的分娩孕周、出生体质量、双胎出生体质量差、宫内病死率、新生儿病死率及半年存活率等情况。结果:观察组孕妇宫内两胎病死率、两胎儿出生体质量差均明显高于对照组(P<0.05或P<0.01);观察组胎儿分娩孕周明显早于对照组,大、小胎儿的出生体质量明显低于对照组(P<0.01);观察组中Ⅱ型组新生儿病死率显著高于Ⅰ型组,分娩孕周明显早于Ⅰ型组,且小胎儿出生体质量最低,明显低于Ⅰ型组(P<0.05)。观察组和对照组间新生儿病死率、半年双胎存活率无显著性差异(P>0.05)。结论:不同类型MCDA合并sIUGR胎儿的妊娠结局和预后均不同,其中Ⅱ型预后差,胎儿宫内病死率高,因此临床需密切监测孕期胎儿情况,及时警惕各种异常。
【关键词】单绒毛膜双羊膜囊;宫内生长受限;妊娠结局;预后
单绒毛膜双羊膜囊(monochorionic diamniotic, MCDA)双胎是临床妇产科的常见疾病,其发病率高,病情严重,并发症较多,严重危及胎儿的生命。选择性宫内生长受限(selective intrauterine growth restriction, sIUGR)是单绒毛膜双羊膜囊的严重并发症,有调查显示,sIUGR的发病率高达11%~14%,在一定程度上导致胎儿的围生期死亡率、发病率、神经系统发病率均较高[1-2]。本研究探讨不同类型MCDA双胎妊娠孕期合并症及胎儿妊娠结局预后分析,现报告如下。
1.1 一般资料 选择我院2010年6月至2015年6月期间收治的MCDA双胎并发sIUGR孕妇40例作为观察组,年龄24~42岁,平均(31.2±4.5)岁。根据临床检查将观察组孕妇分为Ⅰ型组20例、Ⅱ型组12例、Ⅲ型组8例。入选标准:符合中华医学会妇科协会制定的关于MCDA和sIUCR的诊断标准[3],经超声检查结合临床症状确诊。另选取同期无合并症的MCDA孕妇40例(80胎)作为对照组,年龄25~42岁,平均(30.2±4.5)岁。排除孕妇双胎输血综合征、双胎贫血-红细胞增多序列征、双胎动脉反向灌注序列征、一胎儿或两胎儿结构畸形及染色体异常等。2组孕妇的年龄、病情及分型等一般资料无显著性差异(P>0.05),具有可比性。
1.2 方法 40例孕妇入院后均实施临床超声检查、综合治疗及护理干预等,观察组患者增加胎儿生长发育监测次数。对于多普勒脐动脉血流检查波形异常的sIUGR孕妇,妊娠28~32周时给予地塞米松,以便促胎肺成熟;根据孕妇和胎儿的情况选择合适的时机终止妊娠,孕妇28周后若超声检查显示羊水过少、胎儿水肿、胎儿病情恶化及静脉导管持续性a波倒置等,需及时终止妊娠。
1.3 观察指标 对比分析2组孕妇、3型组间胎儿的分娩孕周、出生体质量、双胎出生体质量差、宫内病死率、新生儿病死率及半年存活率等情况。两胎儿出生体质量差=(大胎儿出生体质量-小胎儿出生体质量)/大胎儿出生体质量差×100%[4]。
1.4 统计学方法 采用SPSS20.0统计软件分析数据,计数资料比较采用χ2检验,计量资料比较采用t 检验,多组间比较采用方差分析。
2.1 孕妇妊娠结局及胎儿体质量对比 结果详见表1、表2。
表1 2组孕妇妊娠结局和胎儿体质量的对比
注:1)与对照组比较P<0.01
表2 不同型组孕妇妊娠结局和胎儿体质量的对比

注:1)与Ⅰ型比较P<0.05
观察组胎儿分娩孕周明显早于对照组,两胎儿出生体质量差明显高于对照组,大胎儿、小胎儿的出生体质量明显低于对照组(P<0.01);观察组中Ⅱ型组分娩孕周明显早于Ⅰ型组,且小胎儿出生体质量明显低于Ⅰ型组(P<0.05)。
2.2 2组胎儿预后情况对比 结果详见表3。
表3 2组胎儿预后比较
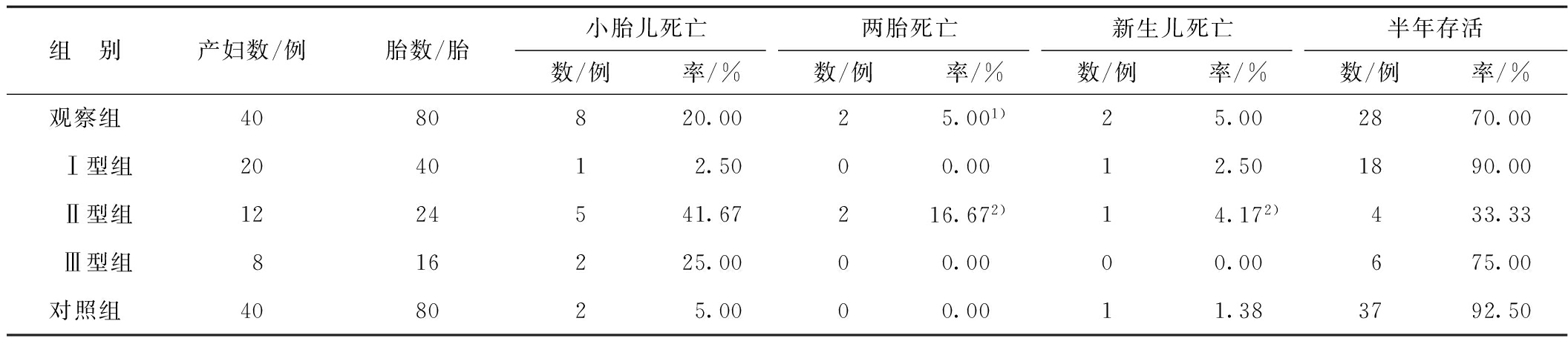
注:1)与对照组比较P<0.05;2)与Ⅰ型比较P<0.05
观察组孕妇宫内两胎病死率明显高于对照组,观察组Ⅱ型组的新生儿病死率为4.17%,显著高于Ⅰ型组的2.50%(P<0.05);但2组新生儿病死率和半年双胎存活率无显著性差异(P>0.05)。
单绒毛膜双羊膜囊 (MCDA)是双胎妊娠中特殊类型,占双胎妊娠率的20%~30%左右。 近年来,MCDA的发病率呈逐年上升趋势。其围生儿患病率和病死率均较高,双胎选择性宫内生长受限(sIUGR)是其严重的并发症之一。有文献报道,sIUGR的分娩孕周显著低于无并发症 MCDA 双胎,sIUGR中总的死胎发生率为 10%,小胎儿死亡后,随后大胎儿死亡的风险高达26%,出现严重神经发育障碍的风险高达 60%[5]。其中sIUGR Ⅲ型孕妇的预后较Ⅱ型好,但较Ⅰ型差[6]。本研究结果亦显示,Ⅲ型组宫内小胎儿病死率、两胎病死率均低于Ⅱ型组,虽然2型间预后各指标无显著性差异,但不排除入选病例较少所致。因此,sIUGRⅠ型胎儿的预后最好,可于孕35~36周时终止妊娠;而Ⅱ型胎儿的病死率较高,需密切监测胎儿的宫内情况,若胎儿未见病情恶化,可将孕周延至32~33周;Ⅲ型胎儿的预后介于中间,可于孕33~34周分娩。故临床上需准确诊断sIUGR及其分型,及时有效地监测和处理[7-8]。
综上所述,不同类型MCDA双胎妊娠孕期合并sIUGR胎儿的妊娠结局和预后均不同,其中Ⅱ型预后差,胎儿宫内病死率高。因此,临床需密切监测孕期胎儿情况,及时警惕各种异常。
参考文献:
[1]门英华,张慧,张焕灵.不同类型单绒毛膜双羊膜囊双胎选择性宫内生长受限胎儿的妊娠结局与预后[J].中国医学工程,2015,23(5):239-241.
[2]王谢桐,李红燕.重视单绒毛膜双胎妊娠的临床研究[J].中华妇产科杂志,2013,48(6):401-404.
[3]KO J K, CHEUNG V Y. Time to revisit the human chorionic gonadotropin discriminatory level in the management of pregnancy of unknown location[J]. Journal of Ultrasound in Medicine, 2014, 33(3): 465-471.
[4]刘新秀,刘子建,王秀美,等.激光凝固胎盘吻合血管术治疗单绒毛膜双羊膜囊双胎并发选择性胎儿生长受限的临床效果分析[J].中华妇产科杂志,2014,49(3):183-187.
[5]ADEGBITE A L, CASTILLE S, WARD S, et al. Neuromorbidity in preterm twins in relation to chorionicity and discordant birth weight〔J〕[J]. Am J Obstet Gynecol, 2004, 190(1): 156-163.
[6]邵长香,孙路明,邹刚,等.单绒毛膜单羊膜囊双胎妊娠17例临床分析[J].中华围生医学杂志,2014,17(9):609-613.
[7]岳洁,刘晓华,卢钺,等.早孕期绒毛膜下血肿的位置与大小对妊娠结局的影响[J].中国妇幼保健,2015,30(34):5983-5984.
[8]FRATES M C, DOUBILET P M, PETERS H E, et al. Adnexal sonographic findings in ectopic pregnancy and their correlation with tubal rupture and human chorionic gonadotropin levels[J]. Journal of Ultrasound in Medicine, 2014, 33(4): 697-703.
Pregnancy outcome and prognosis of different types of monochorionic diamniotic twins with selective intrauterine growth restriction
ZENG Linrui
(Department of Obstetrics and Gynecology, Chengdu Seventh People’s Hospital, Chengdu 610041,China)
【Abstract】Objective:To evaluate the pregnancy outcome and prognosis of different types of monochorionic diamniotic(MCDA) twins with selective intrauterine growth restriction(sIUGR). Methods:40 cases of pregnant women with MCDA twins(80 fetuses) and sIUGR in our hospital from June 2010 to June 2015 were selected as observation group, which was divided into type Ⅰ(20 cases), type Ⅱ(12 cases) and type Ⅲ(8 cases) according to the classification of umbilical artery blood flow spectrum. In addition, 40 normal MCDA cases(80 fetuses) were selected as control group. The gestational week at delivery, birth weight, birth weight difference of twins, rate of intrauterine fetal death, neonatal death and survival rate within 6 months were compared between the two groups, and among the three types of sIUGR as well. Results:Both the rate of intrauterine fetal death and birth weight difference of twins in the observation group were significantly higher than those in the control group(P<0.05 or P<0.01). The gestational week at delivery in the observation group was significantly earlier than that in the control group, and the birth weights of large and small fetuses were also significantly lower than those in the control group(P<0.01). In the type Ⅱ group, the newborn mortality was significantly higher, the gestational week was significantly shorter, and the birth weight of small fetus was significantly lower than those in type Ⅰ group(P<0.05). However, there were no significant differences in the newborn mortality and survival rate within 6 months between the two groups(P>0.05). Conclusion:Different types of MCDA twins with sIUGR demonstrate different pregnancy outcome and prognosis. Of them, the type Ⅱ cases have the worst prognosis and higher rate of intrauterine death. It is necessary to make a close clinical monitoring for the fetus and keep alert for the abnormal conditions.
【Keywords】monochorionic diamniotic(MCDA); selective intrauterine growth restriction(sIUGR); pregnancy outcome; prognosis
【中图分类号】R714.23
【文献标识码】A
DOI:10.11851/j.issn.1673-1557.2017.01.011
优先数字出版地址:http://www.cnki.net/kcms/detail/51.1688.R.20170112.1349.012.html
(收稿日期:2016-05-10)
E-mail:65346325@qq.com